
By Jeffrey W. Chandler, DDS, MD — Elmhurst Oral Surgery
I want to talk to you about something that doesn’t come up enough in dental practice, and that silence has real consequences.
Every single hour of every single day, someone in the United States dies from oral or oropharyngeal cancer. Not every few hours. Not daily. Every hour. Too many people simply don’t know the warning signs, the risk factors, That gap between what’s possible and what’s happening is why I wanted to share or the fact that when this disease is found early, survival rates increase substantially.
Who Gets Oral Cancer? The Risk Profile Has Changed
For decades, the classic picture of an oral cancer patient was a heavy smoker, often male, typically over 50, with significant alcohol use. That picture still exists and remains accurate. Tobacco and alcohol remain the leading risk factors, and their combined use creates a risk far greater than either alone.
But here’s what has changed dramatically in the past two decades, and what I want every patient, including young, healthy, non-smoking patients, to understand: the fastest-growing group of oral cancer patients today are people who don’t smoke and don’t drink heavily. The driver behind this shift is the human papillomavirus, or HPV, specifically the HPV-16 strain, which is now strongly linked to oropharyngeal cancers involving the back of the throat, the base of the tongue, and the tonsils.
In 2024, the National Cancer Institute estimated nearly 58,500 new cases of oral cavity and pharynx cancer in the United States alone. A significant and growing portion of those cases are HPV-related, and they are affecting younger adults who would never have considered themselves at risk.
So if you’re sitting there thinking, “This doesn’t apply to me. I’ve never smoked,” I’d gently ask you to keep reading. One of the most important things I can do as a surgeon who cares deeply about my community is to make sure no one feels falsely protected by the absence of traditional risk factors.
What Your Dentist Should be Looking for During an Exam
Oral cancer screening should not be a separate, formal appointment, it’s best place is to be woven into the examination performed as part of every dental visit. Here’s what I review during an oral cancer screening.
The Head and Neck Assessment
Before I even look inside your mouth, I begin by examining the outside. I carefully feel the lymph nodes in your neck, under your jaw, and along the sides of your throat. Swollen, firm, or fixed lymph nodes can indicate infection, but they can also be among the first signs that something more serious is happening in the head and neck region.
I also visually inspect the skin of your face and lips, looking for any lesions, unusual texture, or discoloration, particularly on the lower lip where prolonged sun exposure is a known risk factor.
Inside the Mouth: A Systematic Examination
Once I move inside, I work through the mouth in a methodical sequence so nothing is missed:
The lips and labial mucosa. I examine both the outer surface and the inner mucosal lining of both lips, looking for irregularities in texture, color, or contour.
The gingiva and alveolar ridges. The gum tissue along both the upper and lower arches is inspected for unusual growths, color changes, or areas of breakdown that don’t follow the pattern of normal gum disease.
The buccal mucosa. This is the inner lining of your cheeks. This is an area patients rarely look at themselves. I stretch and illuminate this tissue carefully. This is a common location for both benign and potentially malignant lesions.
The floor of the mouth. The tissue beneath the tongue is one of the highest-risk sites for squamous cell carcinoma which is the most common type of oral cancer. I use a mirror and lighting to visualize the entire floor of mouth and palpate the underlying soft tissue.
The tongue. I examine the top, the underside, and the sides and base of the tongue, which I ask patients to extend and move so I can see areas that are otherwise tucked away. The lateral tongue borders and the posterior tongue are high-risk zones that deserve careful attention.
The hard and soft palate. I examine the roof of the mouth from front to back, including the soft palate and the uvula. Subtle asymmetry, submucosal masses, or unusual discoloration in this area can be significant.
The oropharynx. Using a mirror and good lighting, I look at the tonsils and the posterior pharyngeal wall for any asymmetry, unusual tissue, or lesions.
What Raises a Red Flag
Most of what I see is normal. But certain findings trigger a closer look and if warranted a biopsy. The changes that concern me most include:
Leukoplakia: white patches on the mucosal surfaces that cannot be wiped away. While many are benign, a meaningful percentage represent dysplasia (pre-cancerous changes) and some are frankly malignant. White patches always deserve investigation, not watchful waiting.
Erythroplakia: red, velvety patches. These are less common than leukoplakia but carry a higher likelihood of malignancy. Red lesions get my attention immediately.
Mixed red and white lesions (erythroleukoplakia): the combination carries a higher risk than either color change alone.
Ulcers that do not heal: any sore in the mouth or on the lip that has been present for more than two to three weeks without a clear explanation deserves evaluation. Trauma-related ulcers heal. Malignant ulcers do not.
Submucosal masses: lumps felt beneath the normal surface tissue that have no obvious explanation.
Numbness or altered sensation: unexplained numbness of the lip, tongue, or other areas of the mouth can signal nerve involvement from an expanding lesion.
Asymmetry in the neck: a lump on one side of the neck that has been present for more than two weeks without explanation should be evaluated.
For HPV-associated oropharyngeal cancers specifically, I also ask about symptoms patients might not associate with their mouth at all: a persistent sore throat that hasn’t resolved, difficulty swallowing, the sensation of something caught in the throat, unexplained ear pain on one side, or a chronic cough. These symptoms, persisting beyond a few weeks, can be signs of oropharyngeal disease.
The Biopsy Conversation
If I find something during an examination that I can’t confidently identify as benign, I will tell you directly. I believe patients deserve a clear, honest explanation of what I see, why it concerns me, and what the next step is. That next step, almost always, is a biopsy which will remove a small sample of tissue for pathological analysis.
I know the word “biopsy” can be frightening. What I try to help people understand is this: a biopsy is not a diagnosis. It is the process of getting a diagnosis. And a biopsy that comes back benign is one of the best phone calls I get to make.
Most oral biopsies are straightforward procedures performed with local anesthesia. The discomfort is minimal and the recovery is quick. The information we gain is irreplaceable.
Wha t You Can Do Between Visits
t You Can Do Between Visits
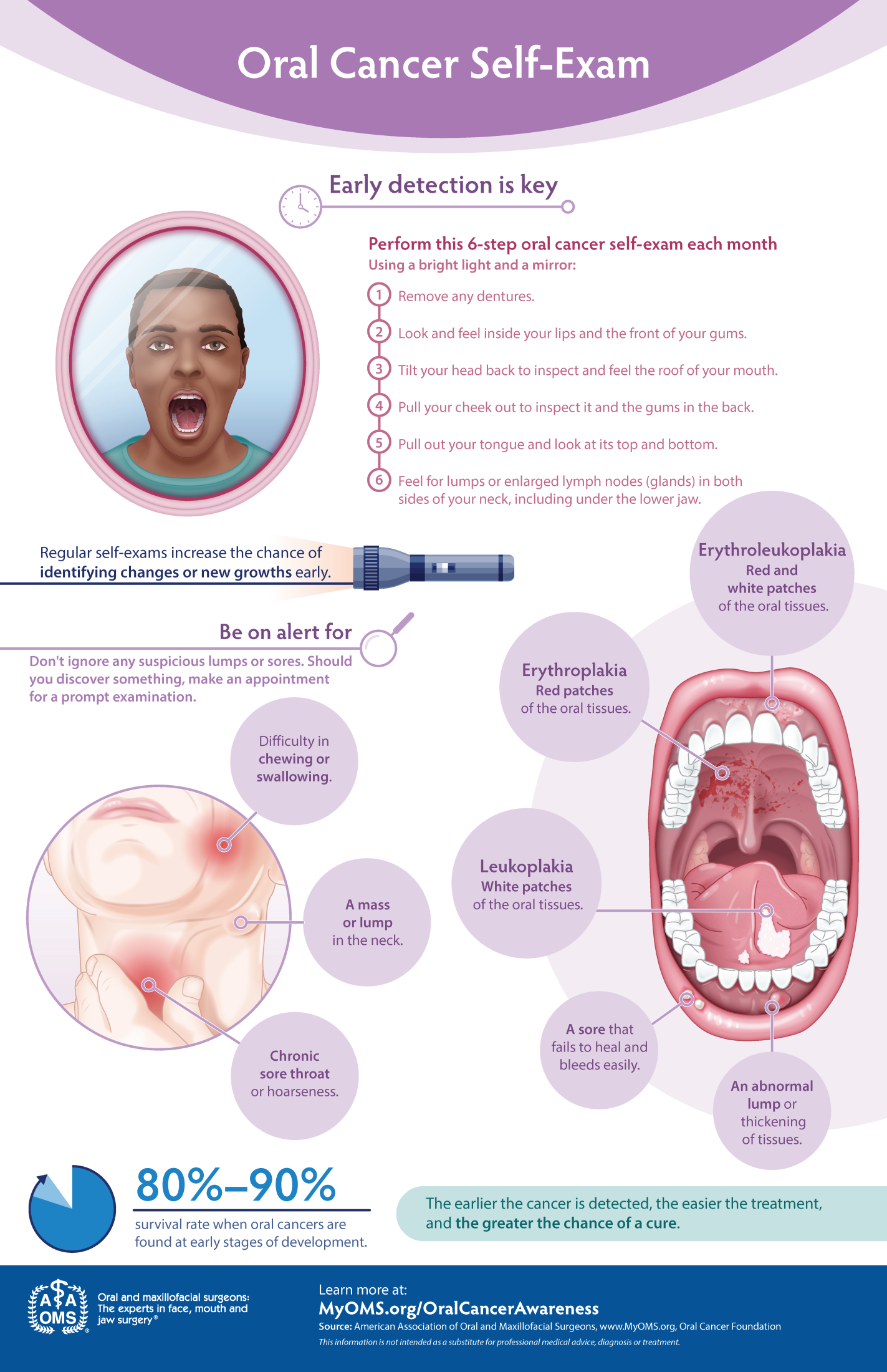
The Oral Cancer Foundation encourages monthly self-exams, and I echo that guidance. You don’t need any special equipment, just a good light, a mirror, and about two minutes. Look at and feel your lips, stretch your cheeks open, extend your tongue and look at the sides, and press gently along the floor of your mouth. If you notice anything that wasn’t there before, a white patch, a red area, a sore that isn’t healing, a lump, give your dentist a call. Don’t wait for your next scheduled appointment.
I also encourage patients who are eligible for the HPV vaccine to speak with their physician about it. The HPV vaccine is one of the most powerful tools we have for preventing HPV-associated oropharyngeal cancers, and it is most effective when given before any exposure to the virus.
A Personal Note
I chose oral and maxillofacial surgery because this specialty sits at a remarkable intersection of medicine and dentistry and we treat some of the most complex conditions affecting the head, neck, and face.
If it’s been more than a year since you’ve had a thorough oral examination, or if you’ve never had a dedicated oral cancer screening, I’d encourage you to talk to your dentist at your next appointment. This is too important to put off.
(630) 833-0395 | elmhurstoralsurgery.com
This content is for general educational purposes and does not constitute individualized medical advice. If you have concerns about symptoms in your mouth or throat, please contact a qualified healthcare provider promptly.